


Homeostatic Control of Osmolarity
Blood osmolarity is one of the most tightly regulated physiological (homoeostatic) parameters, with normal values from 275 to 295 mOsm/kg (mmol/kg). OsM is defined by osmoles of solute per liter where an osmole is one mole of dissolved and dissociated substance in water; hence 1 mole of monosaccharide corresponds to 1 OsM while 1 mole of NaCl is 2 OsM as it dissociates into Na+ and Cl–. OsM is a colligative property and does not depend on molecular size or charge and is only affected by the concentration of dissolved solutes. One mole of glucose in 1 L of water equals 1 OsM, while 1 mole of NaCl is 2 OsM as it dissociates into two ions. OsM increases when dehydrated and decreases when there is too much fluid in the blood. Elevated OsM triggers the production of antidiuretic hormone (ADH) (arginine vasopressin (AVP)) signaling the kidneys to keep more water inside blood vessels concentrating urine; conversely, to decrease osmolality ADH production decreases and blood and urine become more diluted.

Electrolytes are minerals that carry an electric charge and include sodium (Na+), chloride (Cl–), calcium (Ca2+), potassium (K+), magnesium (Mg2+), and phosphate (PO43-). In addition to altering OsM, each electrolyte regulates biochemical pathways involved in protein synthesis, muscle and nerve function, blood glucose control, and blood pressure regulation.
Sodium, the principal cation, maintains normal fluid balance in the body; found naturally in foods and added to certain foods. The daily recommendation of sodium is 1500 mg per day. The average Canadian consumes 3,400 mg/day, double the RDA for sodium. The primary dietary sodium source is NaCl added to packaged, processed, store-bought foods (deli meats, bacon, canned preserves and sauces, salad dressings, bread, and snack foods). Excess salt elevates blood pressure and significantly contributes to heart disease and stroke. Sodium is essential in maintaining cellular osmotic pressure controlling the passage of fluids in and out of cells and transmitting nerve impulses. Chloride, the principal anion, and sodium are responsible for maintaining the osmotic pressure, key in maintaining cell homeostasis and transmitting neuron action potentials. Intake of chloride between 1700 mg to 5100 mg is considered safe; low chloride, relative to sodium, compensates with bicarbonate which can upset the acid-base metabolism. The chloride serum concentration is not homeostatically controlled; chloride concentration passively reflects the concentrations of other ions, especially sodium. Chloride is used in gastric hydrochloric acid secreted from the parietal cells of the gastric mucosa. Potassium is the main intracellular ion essential for maintaining fluid and electrolyte balance. Low potassium increases the risk of hypertension, stroke and cardiovascular disease. Green leafy plants, nuts, seeds and fruits are associated with high potassium concentrations relative to sodium; therefore, crop production rapidly depletes potassium from the soil requiring agricultural fertilizers to remedy its depletion (~90% of the potassium produced globally is used as fertilizer). Potassium RDA is 4700 mg/day for adults.
Calcium is a secondary messenger in signal transduction pathways that release neurotransmitters from neurons, is involved in muscle cell contraction, embryonic fertilization, establishing the electric potential between the interior and exterior of a biological cell, acts as a co-factor for numerous enzymes, and is involved in bone formation. Plasma calcium concentration is tightly regulated, where bone acts as the major calcium reserve when serum calcium levels drop. The resorption of calcium from bone and reabsorption in the kidney into circulation is regulated by the parathyroid hormone (PTH), which increases the conversion of vitamin D to calcitriol, the biologically active form. The RDA for calcium differs with age; for adults, the RDA is 1000 mg/day. Magnesium (Recommended Daily Allowance (RDA) 420 mg) is primarily found in bones, while serum magnesium ranges between 0.75 and 0.95 mOsM; it is used as a co-factor for >300 enzymes, supporting energy production, muscle, and nerve function. Primary sources of Mg2+ are green leafy vegetables, legumes, nuts, seeds, and whole grains, which are added to fortified breakfast cereals. Refining grains removes the nutrient-rich germ and bran, substantially lowering the magnesium.
Since monosaccharides are osmotically active once they enter circulation, they must quickly be removed. In the fasted state, as blood glucose levels decline, the pancreas releases the hormone glucagon, simulating the liver to break down glycogen into glucose. The fed state is much more complex as carbohydrates are not utilized similarly. Carbohydrates differ between glycemic and non-glycemic (fiber); glycemic carbohydrates are available for metabolism providing energy and glucose from sugars and starches, while non-glycemic carbohydrates are neither hydrolyzed nor absorbed in the small intestine and include fibers. Additionally, monosaccharides differ in how they are utilized; for example, fructose does not increase the glycemic response as much as glucose because, during first-pass metabolism in the liver, it simulates hepatic de novo synthesis of fatty acids and, when in excess, can result in fatty liver.
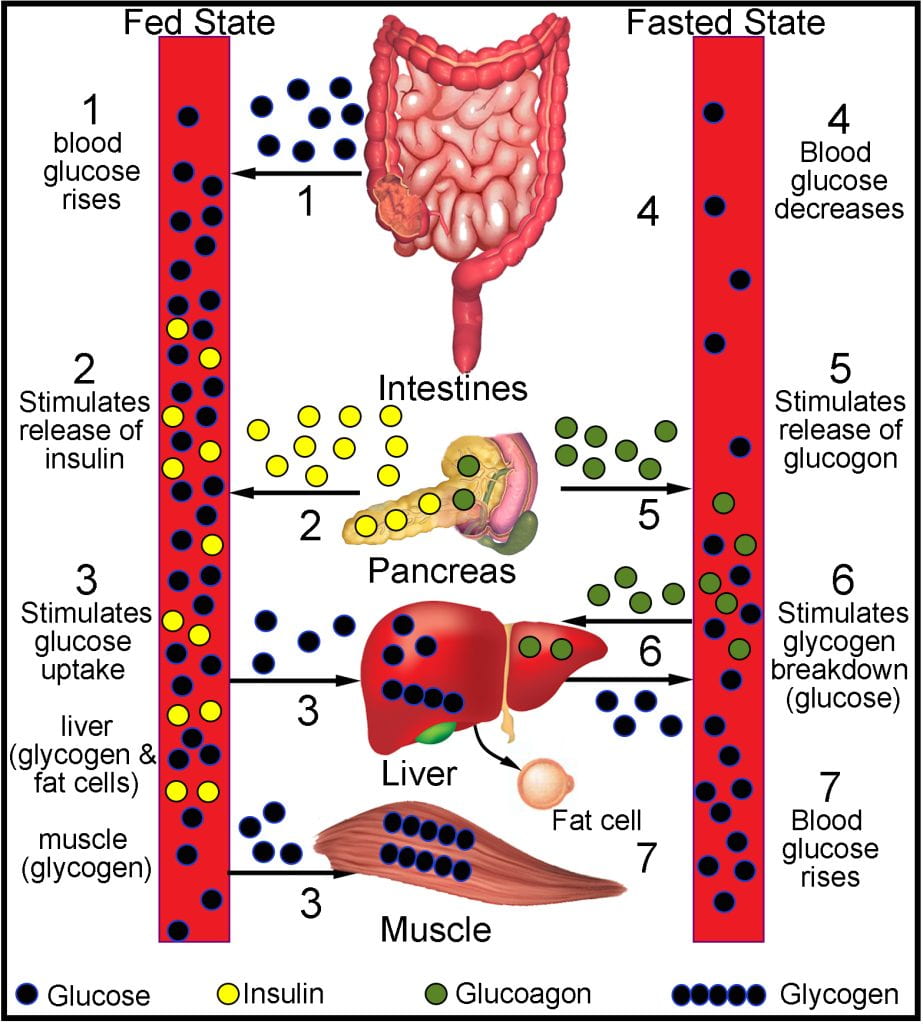
As part of the ileal break, when nutrients are sensed in the small intestine, the hormone glucagon-like peptide-1 (GLP-1) stimulates the pancreas to secrete insulin. The primary cellular mechanism to reduce blood glucose after carbohydrate ingestion utilizes the insulin-stimulated glucose transporter (GLUT4) to shuttle glucose out of circulation and into the skeletal muscle to be stored as glycogen. Macleod & Banting (Nobel Prize 1923) are credited with the discovery of insulin as it was thought to control sugar metabolism, while the lack of insulin caused an increase of sugar in the blood, eventually excreted in the urine. Initial extraction attempts of insulin occurred from homogenized bovine pancreas cells but were unsuccessful because the proteolytic enzymes of the pancreas destroyed insulin; the first source of insulin was extracted from the pancreas of fetal calves. Biosynthetic human insulin, its analogs and its derivatives are produced via gene technologies. Since 1983, biosynthetic forms of insulin have been produced using recombinant DNA technology to insert the human insulin gene into the bacterium DNA, typically either E. coli or Saccharomyces cerevisiae, allowing the “recombinant” micro-organism to produce the insulin protein encoded by the human gene via fermentation.; herein lies the importance of genetically modified organisms (GMOs).
Carbohydrate Digestion and The Glycemic Response
Due to differences in the digestibility of carbohydrates, total carbohydrate is not a good nutritional characteristic; instead, foods are assigned a glycemic index (GI) which is the blood glucose-raising potential of food compared to either white bread or glucose (GIglucose/GIwhitebread ~ 1.4). The glycemic index indicates the physiological function of the carbohydrates consumed from a particular food to raise blood glucose. Ideally, slow, gradual digestion, absorption, and transport of glucose are desired as indicated by a low glycemic index; food that rapidly digests and high-in-sugar or highly digestible starches cause high spikes in blood glucose. The diabetes epidemic is routed by a high intake of refined carbohydrates (e.g., white rice); and dramatically decreased physical activity levels (Hu, 2011). The Western diet, high in simple sugars and highly refined carbohydrates, in addition to a sedentary lifestyle, explains and is ultimately the solution for a characteristic pattern of chronic diseases that emerge in populations as they adopt a sedentary, westernized way of life and diet (O’Dea, 1992). As early as 1985, it was well established that ultra-processed foods produced a higher glycemic index (p < 0.05) than unprocessed foods (Brand et al., 1985). Unprocessed carbohydrate-rich foods, including boiled rice, sweet corn, and potato, induced a lower glycemic response than similar ultra-processed foods, including instant rice, rice Bubbles, corn chips, Cornflakes, and instant potato (Brand, 1985).
Insulin and Diabetes
Type I diabetes mellitus is insulin-dependent “juvenile-onset,” where the pancreas produces insufficient insulin, while type II non-insulin-dependent diabetes mellitus arises as insulin becomes less effective at stimulating to GLUT4 transporter to shuttle glucose into skeletal muscle and is typically characterized as “adult-onset.” However, Type II diabetes is now observed in preadolescent populations. In Canada, 90% of diabetes incidence is Type II, requiring supplemented insulin, which contains 51 amino acids and a molecular weight of 5808 Da, to maintain blood glucose. A third type of diabetes arises during the second or third trimester of pregnancy (gestational diabetes), of which early diagnosis and treatment are paramount to ensure the health of the mother and baby. Individuals with gestational diabetes are not diabetic pre-pregnancy and typically subside postpartum. Untreated gestational diabetes causes preeclampsia or high blood pressure during pregnancy, abnormal sugar levels in the fetus, and often leads to cesarean births due to larger birth weights, increasing the risk of birth injury due to the size and difficulties during delivery.
Although the body responds in each acute exposure by lowering blood glucose, chronic effects of spikes in blood glucose eventually desensitize the GLUT4 receptor to insulin, leading to Type II Diabetes. Insulin lowers blood glucose and controls other aspects of metabolism, such as converting fat into glucose and glucose into fat. Diabetes (diabetes mellitus) is defined by higher-than-normal glucose levels in the blood; failing to control blood sugar levels leads to loss of vision, and diseases of the arteries, the kidneys, and the heart. In 2019, Diabetes Canada released a 360o Roundtable summary report stating, “11 million Canadians are living with diabetes or prediabetes. Treating the disease will cost our healthcare system nearly $30 billion this year. Diabetes rates rise at 40% per decade and show no signs of slowing down.” Diabetes statistics Canada estimates that by 2025 12% of the population will be diabetic, and 23% will be prediabetic, representing a 44% increase between 2015-2025!
Lipid Digestion, Lipoproteins, and their Health Effects
Lipid digestion produces fatty acids and 2-monoglycerides (2-MAG), which are incorporated with other surface active molecules into mixed micelles as they transit through the small intestine. Triglycerides and cholesterol are hydrophobic and insoluble in water, the primary component of blood, and must be transported as lipoprotein assemblies shielded from the water by the phospholipid/apolipoproteins monolayer. At the intestinal epithelial, triglycerides are reassembled from the fatty acids and 2-MAGs and transit via lymphatic circulation as chylomicrons that contain cholesterol, phospholipids, apolipoprotein, and triglycerides. The chylomicron is 85% triglyceride, 7% cholesterol, 5% phospholipid, and 3% protein which are different apolipoprotein (Apo) isoforms that bind lipids.

The exogenous pathway shuttles chylomicrons coated in ApoB48, ApoC and ApoE from the small intestine to the liver, and as it transits, the extracellular enzyme lipoprotein lipase (LPL) found on the vascular endothelial surfaces, hydrolyzes circulating triglyceride-rich lipoproteins, including chylomicrons and very low-density lipoproteins (VLDL). Chylomicrons are removed from the circulation exclusively by the liver using the chylomicron remnant receptor and the ligand, ApoE, found on the chylomicron surface. There are two isoforms of ApoB, ApoB100 synthesized in the liver, consisting of 4563 amino acids, found only on VLDL or low-density lipoproteins (LDL) and ApoB48, produced in the small intestine and found only on chylomicrons, which differs as it has a stop codon at residue 2153 and codes for only 48% of the Apo B100’s sequence.
After reuptake by the liver, cholesterol synthesis occurs and shuttles it through the body to tissues using the reverse transport pathway as high-density lipoprotein (HDL) coated in ApoA, ApoC, and ApoE. HDL transits through circulation, picking up excess cholesterol from tissues while delivering it to those needing cholesterol or other lipoproteins. HDL is often termed “good cholesterol” because it transports lipids and cholesterol out of artery walls and reduces macrophage accumulation, helping prevent or even regress atherosclerosis; however, too much also increases mortality risk. HDL contains 45% protein, 30% phospholipid, 20% cholesterol and 5% triglyceride. The endogenous pathway synthesizes VLDL, coated in Ap0B100, ApoC and ApoE, while circulating fatty acids are cleaved off by LPL, converting VLDL into low-density lipoprotein (LDL). VLDL leaves the liver containing 60% triglyceride, 18% phospholipid, 12% cholesterol, and 10% protein and is then hydrolyzed by LPL during circulation before reuptake as LDL with 10% triglyceride, 22% phospholipid, 45% cholesterol, and 23% protein. LDL that is not taken up by the liver binds to scavenger receptors on macrophages which turn into foam cells and deposit on the artery wall as plaque (atheroma); hence the term “bad cholesterol.” Plaque is deposited onto the walls of blood vessels, specifically arteries, leading to arterial hardening and narrowing, increasing the risk of coronary vascular disease.
Fatty Acid Composition and HDL/LDL
The shuttling of lipids is complex due to their insolubility; HDL shuttles cholesterol out of vessels while LDL deposits onto plaques; hence the HDL/LDL ratio is a marker for cardiovascular disease risk. Since the first epidemiological observations suggested fatty acid composition alters plasma lipid and lipoprotein patterns (Band et al., 1971), controversy ensured. The first study compared hunters and fishermen from the northwestern coast of Greenland, who predominantly consumed a meat-rich diet high in polyunsaturated fatty acids (cold water fish, seal, whale, etc.) and were found to have most types of blood lipids decreased, compared with Danish controls and Danish who emigrated from Greenland to Denmark. The findings were extrapolated to explain the low incidence of ischaemic heart disease and the absence of diabetes in the Greenlandic population. In 2015, a meta-analysis of almost 50 years of research comparing saturated unsaturated (mono- and polyunsaturated) fatty acids was compiled (Hooper et al., 2015). The major findings reported in the Cochrane Review were: 1) less saturated fat, long-term, reduced the risk of cardiovascular events by ~17%; 2) reduced saturated fat intake reduced the risk of myocardial infarction; and 3) fewer cardiovascular events occurred when saturated fat is replaced with polyunsaturated but not monounsaturated lipids.
Metabolic Syndrome

Non-communicable diseases (i.e., cancer, diabetes mellitus, cardiovascular diseases), all of which are related, in part, to diet, are now responsible for a larger percentage (46.8 %) of the mortality rate than communicable diseases (41.0 %) (World Health Organization, 2011). The Western diet has led to the development of an entirely new form of malnutrition, unheard of less than a century prior, as affluent populations have double-digit percentages of individuals diagnosed with metabolic syndrome (MetS). Obesity is fundamental to MetS, as it precedes the emergence of impaired insulin sensitivity, dyslipidemia, hypertension and a 1.6-fold increase in mortality.
Metabolic syndrome increases the risk of heart disease, stroke and type-II diabetes and is defined when three or more of elevated blood pressure, high blood sugar, excess body fat around the waist, and abnormal cholesterol or triglyceride levels occur concurrently. Estimates put the number of Canadian adults as 1 in 5 (Diabetes Canada, 2019). Numerous large cohort studies show that diets high in UFPs concur with a higher incidence of non-communicable diseases. The average Canadian consumes 48% of their calories from UPF. Diets high (>74.2 % calories from UFPs) were associated with higher BMI, greater waist circumference and abdominal obesity (Juul & Hemmingsson, 2015). UPFs are central to the development of MetS as individuals who consume the highest quintile of UFP have a significantly higher body-mass index and odds of being obese than those in the lowest quintile of UFP consumption (Louzada et al., 2015).
Works Cited
Bang, H.O. et al., 1971. Plasma Lipid And Lipoprotein Pattern In Greenlandic West-Coast Eskimos. The Lancet. 297: 1143-1146.
Brand, J.C. et al., 1985. Food Processing and the Glycemic Index. The American Journal of Clinical Nutrition. 42:1192-11956.
Hu, F., 2011. Globalization of Diabetes: The role of Diet, Lifestyle and Genes. 34: 1249-1257.
O’Dea, K. 1992. Diabetes in Australian aborigines: impact of the western diet and lifestyle. Journal of Internal Medicine. 232: 103-107.
Diabetes Canada, 2019. Diabetes 360o: a Canadian call-to-action Roundtable meetings summary report. https://www.diabetes.ca/DiabetesCanadaWebsite/media/Advocacy-and-Policy/Advocacy%20Reports/Compilation-Report-Diabetes-360-Strategy_FINAL.pdf
Hoper, L. et al., 2015. Reduction In Saturated Fat Intake For Cardiovascular Disease. Cochrane Database of Systematic Reviews. Issue 6. Art. No. CD011737.
Juul, F. & Hemmingsson, E. 2015. Trends in consumption of ultra-processed foods and obesity in Sweden between 1960 and 2010. Public Health Nutrition. 18: 3096-3107.
Louzada, M.L., et al. 2015. Consumption of ultra-processed foods and obesity in Brazilian adolescents and adults. Preventive Medicine. 81: 9-15.
World Health Organization. 2011. Global Status Report on Non-communicable Diseases 2010. In A. Alwan (Ed.), WHO Library Cataloguing-in-Publication Data. pp. 1-16. Geneva, Switzerland World Health Organization.